The Challenge: The world has been going through a pandemic involving coronavirus SARS-COV-2, also known as COVID-19. Governments worldwide have implemented measures to stop the spread of the virus, typically through physical lockdowns and recently with vaccines. As soon as they became readily available, several countries like the United States and Canada underwent mass vaccination campaigns for their citizens. As more people were getting the vaccine and together with lockdowns, it seemed that COVID-19 cases in those countries appear going down. But recently, there has been a spike in COVID-19 cases in various places. Let’s take a look at this chart showing COVID-19 cases in a select number of countries Since May 2021 after the vaccination has been carried out for a few months:

Several of the countries noted above are considered leaders in the distribution of vaccinations to their citizens. However, we see that around June 4, case numbers in the United Kingdom were rising. Case numbers in that country have dropped recently but are still much higher than in other countries except Spain. We later see other countries like France, Israel, and the United States have sharp increases in the number of cases later in July. If the vaccine is effective against COVID-19 and its distribution is successful in many countries, why are the case numbers still increasing as before?
People are still catching and spreading it after vaccination
Many shreds of evidence showed that the vaccine protects people from the most severe symptoms, but it does not mean you can’t catch and spread it. Infections amongst fully vaccinated people are known as breakthrough infections. Those with breakthrough infections are often less symptomatic, recover more quickly, and are less likely to pass it on. While such breakthrough infections are relatively mild right now, medical experts are concerned that there may be fully vaccinated people with more severe symptoms in the future, leading to a breakthrough disease.
Let’s also take a look at some data relating to COVID-19 cases in Ontario, Canada:
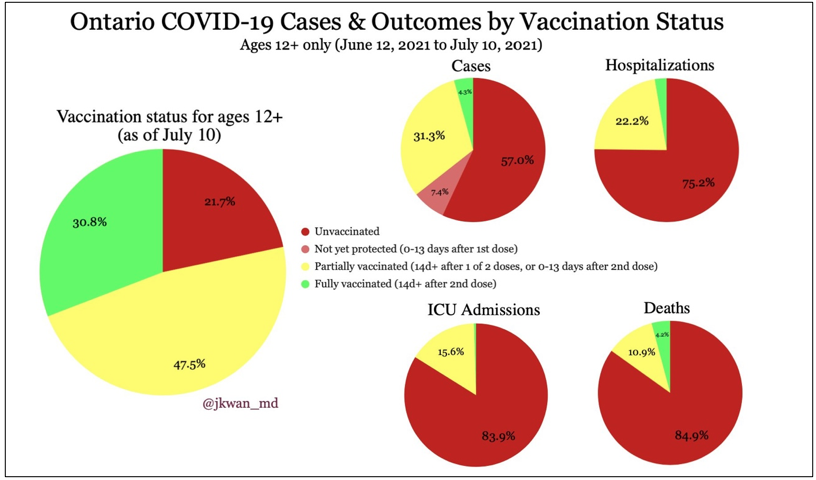
We see that most people from Ontario, Canada, have received at least one dose of their vaccination (47.5% partially and 30.8% fully, total 78.3%). Looking at the number of cases, more than half of new cases are from unvaccinated people, but they only make up 57% of the new cases thus far. The remaining demographic are those that did go for the vaccine: 7.4% are those that got their shot within 13 days, 31.3% are those that are partially vaccinated – one dose after 13 days or two doses within 13 days of the second, and 4.3% are those who are fully vaccinated – two doses with 14 days after the administration of the second dose. So, it seems that those who were vaccinated had just as much of a chance to catch COVD-19 as those who were unvaccinated. Not to mention that each dose needs at least 13 days to inoculate in the body. So, those receiving a single dose have the same protection against unvaccinated people for 13 days after the first administration. Likewise, those receiving a second dose have the same protection as those considered partially vaccinated (13 days after administration of the first dose).
However, when looking at the charts relating to hospitalizations, ICU admissions, and deaths, most COVID-19 cases falling under those are from unvaccinated people. However, even with vaccination, there is still a chance for hospitalization, ICU admission, or death to happen, particularly when a person is only partially vaccinated. Oddly enough, amongst the COVID-19- related deaths, a little over 4% were from people who were fully vaccinated.
One may think that’s this shows how crucial it is to get fully vaccinated with two doses as soon as possible. That is a fair point, given that the protection granted is very effective against the worst of the virus. But the smaller number of people who caught COVID-19 after being fully vaccinated might also come from the reason that there are relatively fewer people who have taken two shots so far. Remember, not too long ago, it was considered enough to just get one dose of the vaccine. Then, it became two doses. Now, there is a possibility that booster shots will be needed. Such booster shots are now seen in Israel, where they are currently granted to its elderly citizens (60 and over). Many other countries are now debating the need to administer booster shots to their citizens, which seems plausible considering how long the vaccine antibodies remain effective. This booster shot may need to be administered to people annually, much like the flu shot. This constant change in information, although understandable, can make the true effectiveness of the vaccine questionable.
There are also cases where a significant number of fully vaccinated people (with two doses) catch the disease. For example, during the July 4 weekend in the United States, a COVID-19 outbreak occurred in Barnstable County of Massachusetts. The Centers for Disease Control and Prevention (CDC) noted that of 469 infections, 74% of them were from people who were already vaccinated with two doses. Of those vaccinated, 79% showed symptoms, and 90% of those cases, approximately 133 people, had the Delta variant. Only five were hospitalized, and there were no deaths. (Source: https://www.cnbc.com/2021/07/30/cdc-study-shows-74percent-of-people-infected-in-massachusetts-covid-outbreak-were-fully-vaccinated.html)
Here’s another piece of data showing the vaccination rate for the state of Massachusetts as of recent:

We see that approximately 64% of people in Massachusetts are fully vaccinated. So, using the data from this and the article mentioned earlier, let’s assign the following values:
People fully vaccinated in Massachusetts = 0.64P; other people = 0.36P;
Sick people that were fully vaccinated =0.74Q; other people = 0.26Q;
Where, P and Q are merely constants the make up the number representing people who got COVID-19 or not amongst the vaccinated and unvaccinated, respectively. However, they will cancel out, considering that we are looking for the ratio of people who got COVID-19 to those who didn’t for the vaccinated or unvaccinated groups. Now we determine the ratio of the percentage of fully vaccinated people who had COVID-19 that weekend to the number of vaccinated people that did not. The same will be done for unvaccinated people who got COVID-19 that weekend to unvaccinated people that did not.
0.74Q/0.64P : 0.26Q/0.36P
This leaves a ratio of 1.156: 0.722, leading to a 1.6:1 ratio between vaccinated people getting COVID-19 to unvaccinated people getting COVID-19. This shows that those who were fully vaccinated had a 60% higher chance of catching COVID-19, regardless of severity.
The chance of these infections post-vaccination may increase as time goes on. The reason for this to happen is still unknown. One of the reasons might be the vaccine is not working as we all expected it should at all.
Variants everywhere
As you may know, SARS-COV-2 has mutated into several variants. These variants result from mutations during the virus’ replication, which causes changes in the virus’s genetic code and how it is received in the body. In SARS-COV-2’s case, the new variants, like the B.1.1.7 (Alpha) and the new B.1.617.2 (Delta), seem to have changes to their spike proteins that bind to a cell’s receptor. With each new mutation, there is always a chance for the virus to replicate into something that can entirely evade the immune system even when one is vaccinated.
As of this article, the most dominant variant is known as the Delta variant, which is known to be more contagious than the variants that came before it. Although vaccines have thus far been effective against COVID-19 and its variants, they seem to have lower effectiveness in protecting the body against the Delta variant, particularly when someone only has one dose. Israel, a leading nation in vaccine distribution, has found that the one doze of Pfizer vaccine was only 39% effective against the Delta variant. However, it was still effective in preventing the most severe versions of the illness. While this is a unique decrease in the vaccine’s effectiveness, other studies have shown similar trends. One study from Public Health England showed that people were still susceptible to COVID-19 and its variants even when vaccinated. The study showed that a single dose of either Pfizer or AstraZeneca only had an effectiveness of 30.7% against the Delta variant. While two doses provided much more protection, the AstraZeneca vaccine was 67% effective against the Delta variant, while the Pfizer vaccine was 88% effective against the Delta variant. So right now, the Pfizer vaccine is still very effective against COVID-19. But the study did show that the effectiveness against the Delta variant (88%) is lower than a 93% effectiveness against the Alpha variant.
Furthermore, new data has shown that the Pfizer vaccine wanes in effectiveness after eight to six months for one or two doses, respectively. So, this means that in the future, additional booster shots may be required. And with the creation of new variants, how long will it be until the acclaimed Pfizer vaccine or any other vaccine becomes totally ineffective?

mRNA vaccines: The vaccines and the time for clinical testing
If you got a vaccine, you would have likely received either the Pfizer or Moderna vaccine, both of which are known as messenger RNA (mRNA) vaccines. These types of vaccines produce an immune response by transferring synthetic RNA into the cells within the person’s body. This causes the cells to build a protein found in specific pathogens and allow the protein molecules to create an adaptive immune response, teaching the body to fight a virus or any other pathogens. This is the first time that we massively use an mRNA vaccine on humans.
Most vaccines go through clinical trials with three phases that take several years for development and testing. When successful, the researchers apply for permission to manufacture and distribute their vaccines. Even then, quality control is still monitored. The clinical trials for the mRNA vaccines, on the other hand, have been much shorter due to emergency approval around the world. Often, these vaccines go through adaptive trials, where changes in the trial itself are made along the way. While more funding and less bureaucracy did help in speeding up the process, this streamlined process is risky. While the data relating to vaccine development is growing, it is still way too little compared to the research gathered in a typical vaccine trial. There is always the risk of low-quality evidence, hindering the thorough scientific understanding of the virus and its effects on patients. Furthermore, it becomes more dangerous if such products are immediately used in public health care on healthy people after such hasty testing.
Current mRNA vaccines also focus too heavily on the spike protein. While the understanding of COVID-19’s spike protein is what made the current vaccines so successful so far, we’ve already seen how the virus’ variants can mutate and change its spike proteins, making it potentially able to bypass someone’s immune system. Furthermore, there has been a lot of debate because of the spike protein and its cytotoxicity. Some say it is dangerous, causing various degrees of damage to different cells. One example of such is the potential neurological damage caused by cytotoxicity. One study from Philadelphia’s Temple University discussed how the spike protein had a negative impact on the blood-brain barrier and caused a pro-inflammatory response on brain endothelial cells. However, the brain endothelial cells were still considered viable. It should also be noted that cases like these are quite rare, though the risk still exists.
That being said, more research is being done to develop a better vaccine that looks at other parts of the virus that the immune system can identify and target. For example, a California-based company is looking into making a vaccine that targets not only the spike protein but also two proteins within the virus’ interior. But the time needed for that means more time for the virus to mutate. And the results of the clinical trials of future vaccines may not be successful even with the hastened process. In a sense, there are many risks involved with the production of mRNA vaccine for a small reduction in the number of COVID-19 cases.
While COVID-19 is steadily being understood and the vaccines have shown effectiveness thus far, the research behind the vaccines is still too rushed for it to be considered ideal. Because the information regarding COVID-19 and the vaccines still needs to be thoroughly investigated and tested, the vaccines we have right now can still be seen only as a temporary solution and one that may not be ideal.
The death and hospitalizations due to COVID-19 are not high in the broader scope
Unfortunately, COVID-19 has taken a lot of lives, as the disease can potentially become fatal. The current vaccines do help mitigate the worst symptoms of the disease. However, the number of deaths throughout the pandemic, especially recently, is actually relatively small compared to the number of COVID-19 cases amongst the whole population of a given area (region, country, etc.). Even before the vaccines, most people who contracted the disease did not die from them. In fact, most people did not even go to the hospital. Instead, they stayed at home to self-isolate. Further still, many cases were considered asymptomatic. Let’s take a look at the number of COVID-19 deaths in Ontario, Canada, on July 30:

In the table above, the cumulative number of deaths in Ontario, Canada, on July 30 only makes up 1.7% of the total number of COVID-19 cases there, the largest of which were from those who were 80 years old and over. We also see that only 5.1 % of total cases for that day were hospitalized cases, and only one percent entering the ICU.
Now let’s take a quick look at the number of cases and deaths related to COVID-19 in some other countries:

A few countries are outlined (Canada, Israel, US, UK, Peru, Mexico, and Yemen) as sample countries highlighting their fatality rates. However, most countries around the world (colored or grayed) have a low case fatality rate regardless of sheer case numbers, usually around five percent or less. Peru, Mexico, and Yemen (outlined as colored dots) are considered exceptions with slightly higher case fatality rates. But these are outliers, and in time, their COVID-19 fatality rate will go down to the same level as everyone else.
Now let’s look at the death rate over the general population. For example, in Canada Ontario, the number of patients who died of COVID-19 is 6 on July 30, 2021, and 0 on August 9, 2021. The general population of Ontario is 15 million. So, the daily death rate is 0.4 people out of every million population on July 30, 2021, 0 on August 9, 2021, and the average is 0.2 person per million. This daily death is very low comparing to other normal reasons for death. For example, Ontario’s number of total deaths from motor vehicle traffic accidences in 2017 is about 61 out of every million people. This translates to a daily death rate of 0.2 people per million population. The chance for a person to die of COVID-19 is at the same level as car accidences. If a vaccine can further lower this small chance of death, this is negligible in a statistical sense.
The reproduction rate R
In many studies, R represents the ability for any infectious disease, e.g., COVID-19, to spread. This R ranges from 0 to any number, which indicates the following:
- When R=0, there are no new infections, and the disease practically dies out.
- When R<1, one existing infection creates less than one new infection. This means that the disease will likely die out on its own. The smaller R is, the faster the disease dies out.
- When R=1, one existing infection creates one new infection. This means that the disease will be around for some time, but there are no outbreaks.
- When R>1, one existing infection creates multiple new infections. This indicates an outbreak has occurred. The larger R is, the faster the disease spreads out.
Throughout the COVID-19 pandemic, the effective R-values have wavered between <1 and >1. Currently, R>1 in several countries around the world, indicating multiple outbreaks. Even with the vaccinations and/or lockdowns, the R-values only went down temporarily before going back up again during the current outbreaks. Also, R-values were marginally brought down thanks to the economic and social sacrifices people had to make during the lockdowns. But with people getting impatient with the lockdowns, many people, regardless of vaccination status, will start breaking the lockdown rules. As fully vaccinated people can still get COVID-19 and pass it on to others, this will tend to bring R back up again to the point of another outbreak.
R is also too heavily emphasized by governments to determine their policies regarding COVID-19 restrictions. Moreover, R typically indicates the disease’s ability to spread on average across a region. It cannot account for clusters within that region, which then skews the R-value as a whole. For example, there was an outbreak last year, which occurred in a meat factory from a region in Germany, which caused the country’s R-value to rise from about 1 to 2.88. This number increased despite low COVID-19 case numbers. This led to Germany going back into lockdown. These regional outbreaks tend to misrepresent how disease spreads across the country as a whole.
Additional research has shown that other variables play a role in determining how COVID-19 spreads. A country may have a lot of cases, but its R-value can equal 1. So, looking at the number of cases is an important variable. Another variable that comes into play is K, also known as the consistency in the way a disease spread. The larger it is, the more consistency in the way that the disease spreads. It is thus important to look at the conditions for allowing the disease to spread in the first place. Research has shown that most disease transmission comes from a small number of individuals, often through “superspreader events” like mass gatherings. One study from the London School of Hygiene & Tropical Medicine showed that COVID-19 had a K value of only 0.1, indicating that 80% of transmissions are caused by 10% of infected individuals. Therefore, it seems the implementation of social distancing, restrictions on mass gatherings and indoor activities, and effective contact tracing (where applied) are what help prevent the massive spread of COVID-19, preventing R from rising. The vaccines can provide some protection, but if a vaccinated person attends an event that could be considered a “superspreader event”, then they will get COVID-19 anyways.
Costs
The general public does not pay for the vaccine. Vaccination providers cannot charge you for the vaccine, any administrative costs, or require additional services that may be billed. They also cannot deny someone vaccination due to lack of health insurance, But the vaccine is not charity work, as there are many upfront costs related to the development of the vaccines in the first place. Most of the money goes into the research and development of the vaccine. Other costs go into the manufacturing, quality control and assurance, sales, and distribution of the vaccines. This adds up to a high upfront cost, which governments worldwide pay to get the vaccines from these pharmaceutical companies. As a matter of fact, governments worldwide invest a lot of money in these pharmaceutical companies for the production and distribution of vaccines to the country. The United States, a leading investor, has invested billions of dollars in pharmaceutical companies for the production and distribution of vaccines. Starting last year, the United States government undertook a partnership with other pharmaceutical companies known as “Operation Warp Speed”, funding the development, manufacturing, and distribution of the COVID-19 vaccines we know now. The funding for this partnership was initially ten billion dollars, later rising to 18 billion dollars. Where do governments get the money for this? Through the people’s tax dollars. So technically, it is not exactly free.
Time is also used up when getting the vaccines distributed and administered to the citizens. Even with the hastened process for clinical testing, it still took more than a year to develop the first vaccines. The distribution of these vaccinations also takes time to reach their destination, which is seen as they are flown across the globe. Then, once they get into the country, they need to be sent to designated clinics like vaccination clinics or pharmacies. Time is also invested in training staff and volunteers.
As for people receiving the vaccination, they have to take time off their busy schedules to go to the designated clinic. It takes to get the shot, much of which is spent waiting to see if any allergic reactions occur. Moreover, many people must take time off work (at least one day) to recover from the vaccine’s side effects. This means that companies lose time on productivity. In certain countries like Canada, the government reimburses such companies with the employees’ wages up to a certain number of days, providing that an employee is away due to COVID-19-related reasons like getting the vaccine. But of course, this means more money spent by the government.
Side effects
All vaccines, regardless of their type, have side effects. The COVID-19 mRNA vaccines also have their own side effects, which include:
- short term: fever, headache, loss of appetite, tiredness, nausea, and muscle pain
- long term: possible affecting existing chromonic diseases, blood related issues, neurological issues, immunization system issues, reproduction related issues, genetic diseases, cancers, and/or unknown problems.
However, the severity of the side effects varies from person to person. For the most part, they are typically mild and show that the body has an immune response. Many people may need to rest for a full day after the shot to recover. But with some other people, the side effects can be more severe, causing illness for three days or more. This relates back to how time is lost because the person needs to rest for a certain number of days.
More severe side effects have been noted since vaccinations began. These symptoms are rarer, but when they do happen, the safety of the vaccine becomes questionable. For example, the AstraZeneca vaccines were known to cause blood clots and low platelet count after receiving the vaccination. The blood clots can appear anywhere within the body, including the brain. The reason for this happening is not clear; it is possible that someone’s immune system might create antibodies that react with the platelets, causing the blood clot to occur. The clots appear to also happen long after receiving the vaccine, up to 42 days after receiving a dose. While this vaccine brand is the most known for this, studies have recently shown that the Pfizer vaccine also carried a risk of causing blood clots as well. A study from Oxford University shows that the blood clot is just as likely with the Pfizer and Moderna vaccines (4 in 1 million chance) as it is for the Astrazeneca vaccine (5 in one million chance). The chance of it happening was extremely rare, regardless of vaccine choice, but present nonetheless. Another extreme side effect seen in some patients that take vaccines is myocarditis, the inflammation of heart muscles.
Research has also shown that these particular vaccines can create adverse neurological effects. The study mentioned earlier regarding the effects of the vaccine’s spike protein on brain endothelial cells, and the blood-brain barrier is one such example. Additionally, several clinical trials have shown that the main vaccines – Pfizer, Moderna, and AstraZeneca – show many participants that developed neurological disorders. Let’s take a look at the adverse effects shown in participants during Pfizer’s clinical trials:


The majority of the adverse effects from vaccines during clinical trials were general disorders, approximately 18%. However, the trials show a surprising number of participants (1158 cases or 6.8%) developing neurological disorders after getting the vaccine.
Clinical trials for the Moderna vaccine have also shown a fairly high number of neurological disorders compared to other adverse effects, as shown in the following table:

The table shows that amongst all the adverse effects present during clinical trials, nervous system disorders were prevalent in 4.1 % of all participants, just below the more common general disorders (5.9%). Fortunately, there were not nearly as many participants that showed severe symptoms.
The tables above also seem to show other symptoms in participants that fall outside the standard symptoms (headache, fever, etc.). Overall, while nervous disorders and other outlying symptoms are less likely to occur to someone during vaccination, it is not a guarantee that they won’t get it either. Furthermore, severe side effects are more likely in people with health complications, such as a compromised immune system. People with such health complications may not even be able to get the vaccine because of the higher risk and/or severity of the side effects in those individuals.
Face masks
Even with full vaccination, governments/CDC are still requiring people to wear face coverings or face masks. As noted before, it is still possible for a vaccinated person to catch the disease. The majority of people that do contract COVID-19, whether they are vaccinated or not, are asymptomatic. Not only does this make contract tracing a lot harder, but a fully vaccinated asymptomatic person could also still spread the disease to another person no matter if he/she is vaccinated or not. By wearing a face mask, even if you are fully vaccinated and/or asymptomatic, the face mask will help prevent it from spreading to other people, and/or prevent you from catching COVID-19 and other diseases too. But it should be noted that even with a face mask, there is a chance of catching COVID-19 because openings on the side still allow the virus to enter. This side opening problem can be solved by using a novel electrically heated face mask recently developed by Sterviral (Sterviral.com). We were wearing face masks before vaccinations were available, and we are wearing them now. It did not matter whether we had the vaccine or not. Face masks and social distance are proved to be reliably effective and keep the R below 1.0. For any infectious disease to die out, the duration of R < 1.0 needs to be long enough.
Conclusion
So even after this rant, are the vaccines really worth it? COVID-19 vaccines still seem to be effective against the current major viruses at this time. However, the various challenges addressed in this article make the vaccine’s role in the fight against COVID-19 a trickier matter. The payoff is also questionable, considering that a fully vaccinated person can still get COVID-19 in a mild or moderate form. So, while vaccines are still considered a reliable asset against this pandemic in the general public, it is coming to a point where they alone cannot stand against COVID-19.
It should also be noted that despite the world’s desire for mass vaccination, it will be impossible to get every single person vaccinated. Some reasons include, but are not limited to severe reactions due to underlying health complications, the inability to access a vaccine and/or proper medical care, outright untrust, and vaccine hesitancy. Whatever the reason, this will leave a large portion of people without vaccination.
As mentioned earlier, even when fully vaccinated, people are still recommended and expected to wear face masks and practice social distancing. So, if the face masks and social distancing are to continue anyway, why not get something that could prevent you from getting COVID-19 in the first place.
One type of face coverings that can help a lot is an electrically heated face mask (Sterviral.com). This type of device is worn just like a typical reusable face mask. However, the mask can produce a high-temperature thermal barrier around one’s nose and mouth, where pathogens tend to enter and go out. The high temperature can increase airflow to increase oxygen and reduce carbon dioxide and humidity, so to make wearing much more conformable. The thermal barrier can also prevent side leaking plagued by all existing face masks. According to WHO, a temperature above 60°C can kill coronaviruses. There was also one study from the University of Hong Kong that shows that the COVID-19 viruses were killed after 5 minutes at 70oC. The electrically-heated face mask can heat up to a temperature as high as 90 oC, which will kill any pathogens around the nose and mouth areas more quickly.